")

Uterine Tumor
Concepts Of Endometrial Cancer Management
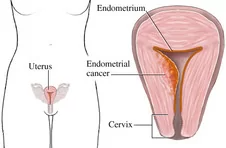 Picture Endometrium is the inner lining of uterus (womb). Endometrial cancers are seen mainly in the postmenopausal women. It presents with abnormal vaginal bleeding, pelvic pain & weight loss. Diagnosis is confirmed by an endometrial biopsy (dilatation & curettage). This biopsy gives a guideline about the extent of surgery required. Imaging (CT or MRI) is required to plan the surgery.
Picture Endometrium is the inner lining of uterus (womb). Endometrial cancers are seen mainly in the postmenopausal women. It presents with abnormal vaginal bleeding, pelvic pain & weight loss. Diagnosis is confirmed by an endometrial biopsy (dilatation & curettage). This biopsy gives a guideline about the extent of surgery required. Imaging (CT or MRI) is required to plan the surgery.
Type of Surgery Based on Histology & Extent of Disease:
|
Histological Type |
Surgical Extent |
| Low grade (endometroid ) without cervical involvement | Total hysterectomy & bilateral salpingo- oophorectomy with or without pelvic & paraaortic lymphadenectomy |
| Low grade (endometroid ) with cervical involvement | Radical Hysterectomy (like Cervical Cancer), bilateral salpingo- oophorectomy, pelvic & paraaortic lymphadenectomy along with peritoneal cytology |
| Low grade (endometroid ) with extra-uterine disease (omental, nodal, rectum, peritoneal, etc.) | Total hysterectomy, bilateral salpingo- oophorectomy, pelvic & paraaortic lymphadenectomy, debulking. |
| High grade (clear cell, papillary serous & carcinosarcoma) | Comprehensive Surgical Staging (like Ovarian Cancer): Total hysterectomy, bilateral salpingo- oophorectomy, pelvic, paraaortic lymphadenectomy, peritoneal cytology, omentectomy & complete cytoreduction. |
All the above surgeries have been traditionally performed using abdominal incision. Standard abdominal hysterectomy for early stage endometrial cancer is an effective and accepted treatment in patients with early stage endometrial cancer. However, pelvic & paraaortic lymphadenectomy is performed in-order to give better clearance. Treatment options for endometrial cancer differ according to the disease status (Table) and vary from a primary surgical treatment to a combination of surgery and adjuvant radiotherapy or chemotherapy or hormonal therapy. Adjuvant therapy in the form of radiotherapy, chemotherapy & hormonal therapy would be required based on the findings on final histopathology.