")

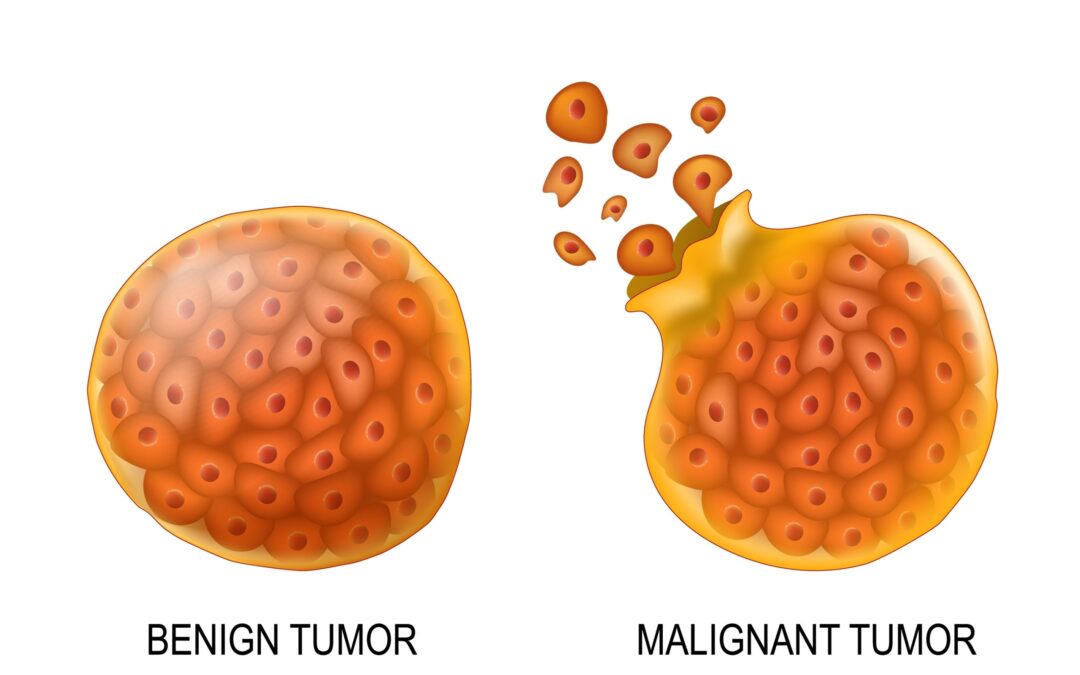
Doctors differentiate benign from malignant tumours through imaging characteristics, tissue biopsy under a microscope, growth pattern observation, and testing whether the tumour invades surrounding tissue or spreads to distant organs. Benign tumours grow slowly inside a capsule with well-defined borders and cells that look like normal tissue. Malignant tumours grow rapidly with irregular borders, disorganized cells, and the ability to invade locally and metastasize through blood and lymphatic channels.
According to Dr. Sandeep Nayak, Best cancer treatment in Bangalore, “Patient gets an ultrasound showing a lump and the report says ‘probably benign’ with a recommendation for follow-up. Family reads ‘probably’ and panics. Or worse, they read ‘benign’ and relax completely. Neither reaction is right. Only a biopsy tells you what the lump actually is. Imaging guesses, pathology confirms.”
Imaging suspects. Biopsy confirms. That’s the order that matters
How Do Doctors Tell Them Apart?
No single test gives the answer alone. Diagnosis follows a sequence from imaging to biopsy to pathology, each step narrowing the probability until the microscope delivers the final verdict.
- Imaging clues: Benign tumours appear well-defined, smooth-bordered, homogeneous on ultrasound and CT. Malignant tumours show irregular margins, heterogeneous texture, and surrounding tissue infiltration. Imaging raises or lowers suspicion but cannot confirm malignancy by itself.
- Biopsy under microscope: Gold standard. Pathologist examines cell shape, arrangement, and division rate. Benign cells look organized and resemble normal tissue. Malignant cells appear disorganized, divide rapidly, and show features like nuclear enlargement and abnormal mitotic figures.
- Growth behaviour: Benign tumours grow slowly, stay encapsulated, push surrounding tissue aside without destroying it. Malignant tumours grow fast, break through their capsule, invade surrounding structures. A lump that doubled in size over three months behaves differently from one unchanged for two years.
- Spread capability: Benign tumours never metastasize. They stay where they started. Malignant tumours send cells through blood vessels and lymphatics to distant organs like liver, lungs, bones, brain. Finding the same cancer in a distant organ confirms malignancy regardless of what the primary looked like.
Your oncologist sequences these investigations through precision diagnostics to reach a definitive diagnosis before any treatment decision.
Can a Benign Tumour Become Malignant ?
Most benign tumours stay benign forever. But specific types carry transformation risk that justifies monitoring or preventive removal.
- Adenomatous polyps: Colon polyps following the adenoma-carcinoma sequence. Left alone long enough a percentage will transform into colorectal cancer over 10-15 years. This is why colonoscopy removes every polyp found and sends it for pathology regardless of how innocent it looks on camera.
- Pleomorphic adenoma: Most common benign parotid gland tumour. Carries a small but documented long-term malignant transformation risk if left untreated for decades. Surgical removal is recommended even though the tumour is benign because waiting invites a problem that removal would have prevented.
- Fibroids rarely transform: Uterine fibroids turning into leiomyosarcoma happens in less than 0.1% of cases. Most women with fibroids will never develop cancer from them. But a fibroid growing rapidly after menopause when estrogen levels have dropped raises suspicion because that growth pattern doesn’t fit the biology of a benign tumour anymore.
- Barrett’s esophagus: Not a tumour but a precancerous tissue change in the food pipe from chronic acid reflux. Annual surveillance endoscopy catches the transition from benign to malignant changes early enough to intervene before cancer establishes itself.
Knowing how liquid biopsy detects cancer DNA in blood at molecular level explains why tissue biopsy under microscope remains the definitive answer for distinguishing benign from malignant when imaging alone can’t decide.
Why Choose MACS Clinic ?
Dr. Sandeep Nayak’s team at MACS Clinic follows the imaging-biopsy-pathology sequence without skipping steps. Ultrasound-guided FNAC or core biopsy happens at the first consultation itself so patients don’t spend weeks in limbo between discovering a lump and knowing what it is.
Lump found here gets a biopsy before the second visit. Because a week of certainty is worth more than a month of “probably benign” sitting on an ultrasound report that nobody followed up.
Call +91 8035740000 to book your consultation.
FAQs
Can imaging alone confirm if a tumour is cancerous?
No, imaging raises suspicion but only biopsy with microscopy confirms malignancy.
Do all benign tumours need removal?
No, most are monitored. Removal is advised when there’s growth, symptoms, or transformation risk.
Can benign tumours spread to other organs?
No, benign tumours never metastasize. Spread to distant organs confirms malignancy.
How long does biopsy take to confirm benign or malignant?
FNAC results in 48-72 hours. Core and surgical biopsy results in 5-7 days.
References
- Benign and malignant tumour differences — National Cancer Institute
- Tumour classification and diagnosis — World Health Organization