")

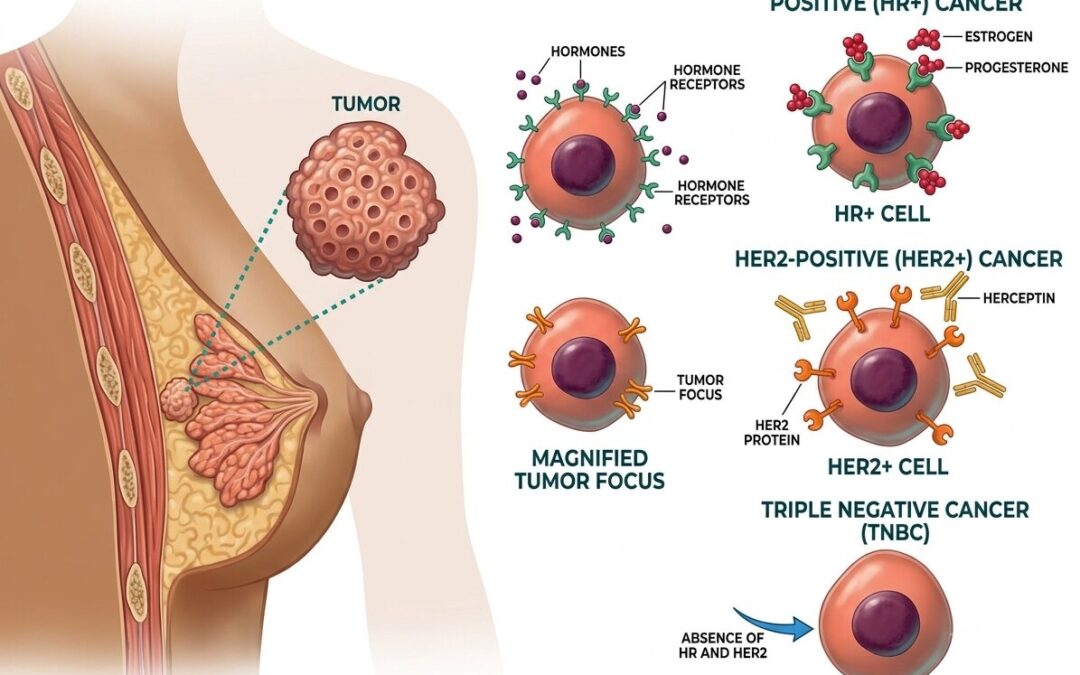
Triple negative breast cancer tests negative for estrogen receptors, progesterone receptors, and HER2. That rules out hormone therapy, aromatase inhibitors, and HER2-targeted drugs entirely. It’s 10% to 15% of all breast cancers, grows faster than receptor-positive subtypes, and carries a higher recurrence risk in the first 3 to 5 years after diagnosis. Chemotherapy is the primary systemic treatment, with immunotherapy now added for high-risk early cases.
According to Dr. Sandeep Nayak who provides, Best cancer treatment in Bangalore, “TNBC is harder to treat not because it doesn’t respond to treatment but because the usual targets aren’t there. Chemotherapy is not a second choice here. It’s the primary systemic treatment and when given correctly with immunotherapy in the right cases, it achieves pathological complete response in close to half of patients.”
No hormone therapy. No HER2 drugs. What does that actually leave for treatment? Quite a bit, if the biology is assessed properly
What Makes Triple Negative Breast Cancer Different?
TNBC doesn’t follow the same biological rules as other breast cancer subtypes. The treatment approach reflects that.
- No Receptor Targets:
Tamoxifen, letrozole, trastuzumab, pertuzumab. None of them work here. Without a receptor to block, cytotoxic chemotherapy is the only systemic option that’s reliably effective across most TNBC cases. - Earlier Recurrence Window:
Most TNBC recurrences happen within the first 3 to 5 years. After that, recurrence risk actually drops. That’s the opposite pattern from hormone receptor-positive cancers, where late relapse beyond 5 years is a real concern. - Brain and Lung Spread:
When TNBC metastasises, it goes to the brain and lungs first. Hormone receptor-positive cancers tend to go to bone. Different biology, different surveillance focus, different complications to plan for. - BRCA Mutation Overlap:
Roughly 10% to 20% of TNBC patients carry a germline BRCA1 or BRCA2 mutation. Worth testing every TNBC patient regardless of family history, because PARP inhibitors are only available to carriers and the mutation rate in TNBC is higher than assumed.
Surgery for TNBC follows the same principles as other breast cancer types. Breast Cancer Surgery approach, lumpectomy or mastectomy, gets decided after neoadjuvant chemotherapy response is assessed.
How Is Triple Negative Breast Cancer Treated?
Without hormone or HER2 targets, the treatment plan relies on chemotherapy, surgery, and immunotherapy in a specific order.
- Neoadjuvant Chemotherapy First:
Anthracycline and taxane-based regimens before surgery are standard. Pathological complete response after neoadjuvant chemotherapy is one of the strongest survival predictors in TNBC. Patients who achieve it have long-term outcomes that approach receptor-positive subtypes. - Immunotherapy Added for High-Risk Cases:
Pembrolizumab combined with neoadjuvant chemotherapy is now standard for early high-risk TNBC following KEYNOTE-522 trial data. PDL1 status is checked but all high-risk early TNBC patients are considered for it regardless. - Residual Disease Escalation:
Patients with residual disease after neoadjuvant chemotherapy get adjuvant capecitabine. This post-neoadjuvant step reduces recurrence risk in patients who didn’t achieve complete pathological response. It’s now built into standard protocols. - PARP Inhibitors for BRCA Carriers:
Olaparib and talazoparib are approved for germline BRCA-mutated metastatic TNBC. These aren’t available to non-carriers. That’s why testing matters at diagnosis, not only when metastatic disease develops.
Our previous blog on Breast Cancer Necessary is worth a read for understanding how surgery fits TNBC treatment and when neoadjuvant chemotherapy changes what the operation needs to achieve.
Why Choose MACS Clinic for Triple Negative Breast Cancer Treatment?
Dr. Sandeep Nayak’s team at MACS Clinic reviews every TNBC case through a tumour board that covers surgical oncology, medical oncology, and pathology before any plan is confirmed. BRCA testing, PDL1 status, and neoadjuvant response are all assessed before surgical planning begins. The operation gets sized to what the tumour is doing after systemic treatment, not what it looked like at diagnosis.
TNBC decisions affect both survival and surgical outcome and they’re time-sensitive. Getting the sequence right requires all disciplines in one room, not separate consultations that don’t talk to each other. Those who want to discuss their diagnosis can reach the team at +91 8035740000.
FAQs
What does triple negative mean in breast cancer?
Triple negative means the tumour tests negative for estrogen receptors, progesterone receptors, and HER2, ruling out hormone therapy and HER2-targeted drugs.
Is triple negative breast cancer curable?
Yes. Early-stage TNBC treated with neoadjuvant chemotherapy and surgery achieves pathological complete response in 40% to 60% of patients, linked to long-term cure rates.
What chemotherapy is used for triple negative breast cancer?
Anthracycline and taxane-based regimens are standard. Pembrolizumab is added for high-risk early TNBC. Capecitabine is used for residual disease after neoadjuvant treatment.
Does BRCA mutation testing matter for TNBC?
Yes. All TNBC patients should be tested regardless of family history. BRCA-mutated TNBC qualifies for PARP inhibitor therapy not available to non-carriers.
Disclaimer: This content is published for educational and informational purposes only.