")

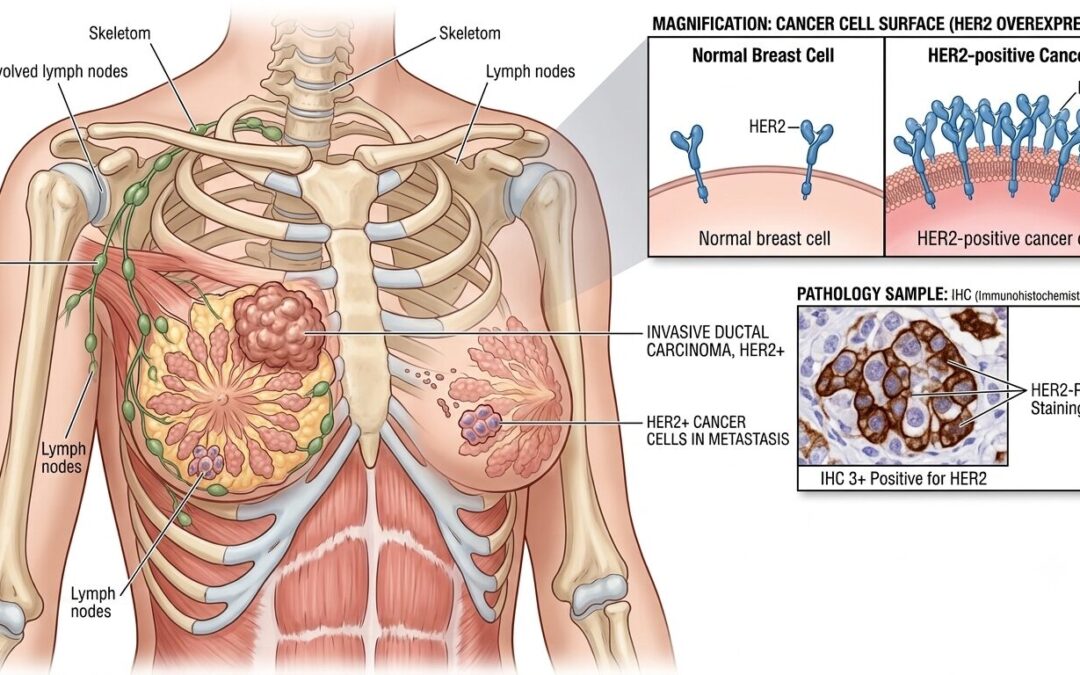
HER2-positive breast cancer happens when tumour cells carry too many copies of the HER2 protein, which pushes cells to divide faster than they should. It’s 15% to 20% of all breast cancers and was once one of the harder subtypes to treat. That changed when trastuzumab arrived. A drug that directly blocks the HER2 receptor cut recurrence risk by nearly half and completely shifted what this diagnosis means for a patient’s long-term outlook.
According to Dr. Sandeep Nayak,who provides Best cancer treatment in Bangalore, “HER2-positive breast cancer is a good example of how identifying the biology changed what treatment could achieve. Trastuzumab cut recurrence risk by nearly half in early HER2-positive breast cancer. The subtype that was once associated with poor outcomes is now one where complete pathological response is achievable in a significant proportion of patients with the right treatment.”
Diagnosed with HER2-positive breast cancer and trying to understand what the treatment actually involves? The biology here is specific and so is the response
What Makes HER2 Positive Breast Cancer Different?
The extra HER2 protein changes how fast tumours grow and which treatments can actually stop them.
- Gene Amplification Drives Growth:
Too many copies of the HER2 gene produce excess protein on the cell surface. That protein acts like a stuck accelerator. Cells keep dividing. Faster than in hormone-positive subtypes, and with less dependence on oestrogen to fuel that growth. - Testing Isn’t Always Straightforward:
IHC gives a score of 0, 1+, 2+, or 3+. Only 3+ is clearly positive. A 2+ result needs FISH testing to check whether gene amplification is actually there. Getting this right matters more than most things because the treatment decision pivots entirely on it. - Half Also Have Hormone Receptors:
About 50% of HER2-positive tumours are also oestrogen or progesterone receptor-positive. Those patients need both anti-HER2 therapy and hormone therapy running in parallel. Addressing only one pathway while the other keeps driving growth is a planning error. - Brain Metastasis Happens More Often:
Of all breast cancer subtypes, HER2-positive has the highest rate of brain involvement in metastatic disease. That doesn’t make it unmanageable but it does change what surveillance looks like and which drugs need to cross the blood-brain barrier.
Surgical planning after neoadjuvant treatment depends on how much tumour remains. Breast Cancer Surgery options get decided once the response is assessed, not before treatment starts.
How Is HER2 Positive Breast Cancer Treated?
Anti-HER2 drugs changed what’s possible here more than almost anything else in breast oncology over the last 25 years.
- Dual Blockade Before Surgery:
Trastuzumab and pertuzumab together with chemotherapy before surgery is the standard for early HER2-positive cases. Two drugs blocking HER2 from different angles at once. Pathological complete response in 40% to 60% of patients. That number matters because pCR predicts long-term survival better than almost any other marker. - T-DM1 When Disease Remains:
Patients who still have tumour after neoadjuvant treatment switch to T-DM1. It’s trastuzumab with a chemotherapy molecule attached that gets delivered directly into HER2-positive cells. The KATHERINE trial showed it cut recurrence risk in half compared to continuing trastuzumab alone. Not a consolation option. A planned escalation. - Extended Adjuvant Therapy:
After trastuzumab, high-risk HR-positive HER2-positive patients get neratinib for a year. It goes after residual HER2 signalling through a different mechanism. Particularly useful for reducing late brain recurrence. Doesn’t suit every patient but worth considering in the right risk profile. - Metastatic Disease Options:
First-line for metastatic HER2-positive is trastuzumab, pertuzumab, and a taxane. Second-line is now trastuzumab deruxtecan, which has shown activity even in HER2-low tumours. The treatment landscape for metastatic HER2-positive disease keeps moving faster than almost any other solid tumour.
Our previous blog on Male Breast Cancer is worth a read. HER2 status and receptor expression drive treatment decisions differently depending on who the patient is, and male breast cancer shows that clearly.
Why Choose MACS Clinic for HER2 Positive Breast Cancer Treatment?
Dr. Sandeep Nayak’s team at MACS Clinic confirms HER2 status through IHC and FISH before anything else happens. Dual anti-HER2 blockade with neoadjuvant chemotherapy, response assessment at surgery, and T-DM1 escalation for residual disease are all part of the treatment pathway. The operation gets planned after systemic treatment shows what it can do, not upfront when the full picture isn’t clear yet.
HER2-positive breast cancer responds well when the sequencing is right. Getting that sequencing right means all disciplines reviewing the case together before the first decision is made. Those who want to discuss their diagnosis can reach the team at +91 8035740000.
FAQs
Can men actually get breast cancer?
Yes, they can. Men are born with a small amount of breast tissue and that tissue can turn malignant. Less than 1% of all breast cancers are diagnosed in men, which is exactly why most men never think to check.
What are the symptoms of breast cancer in men?
Usually a firm lump sitting behind or near the nipple that doesn’t hurt. Some men also notice the nipple pulling inward, discharge, or skin that starts thickening over the chest. None of these feel alarming, which is why they get ignored.
What is the treatment for male breast cancer?
Surgery first, almost always modified radical mastectomy. More than 90% of male breast cancers are hormone receptor-positive, so tamoxifen follows for 5 to 10 years. Chemo and radiotherapy are added when nodes are involved or the tumour grade is high.
Is HER2 positive breast cancer hereditary?
Not typically. The HER2 gene amplification develops in the tumour itself, it’s not something passed down through families. A BRCA mutation can show up in the same patient but that’s a separate issue with its own separate management.
Disclaimer: This content is published for educational and informational purposes only.