")

Robotic parotidectomy is a remote-access surgery that removes tumors from the parotid gland through hidden incisions behind the ear or along the hairline instead of the standard incision running in front of the ear down to the neck. The parotid gland sits just in front of each ear and the facial nerve passes directly through it, making surgery in this area technically demanding regardless of approach. Robotic magnification and wristed instruments allow the surgeon to dissect around the facial nerve branches with precision that reduces the risk of post-operative facial weakness.
According to Dr. Sandeep Nayak, Robotic Parotidectomy surgery in Bangalore,
“Standard parotidectomy leaves a scar right where everyone can see it, in front of the ear running down the neck. Patients come in worried about the tumor and leave worried about the scar. Robotic approach puts the incision where nobody looks.”
Parotid tumor out, facial nerve safe, scar hidden where clothing or hair covers it.
How Is Robotic Parotidectomy Performed ?
Open parotidectomy uses a modified Blair incision running from the front of the ear down into the neck. Robotic approach avoids that visible wound entirely.
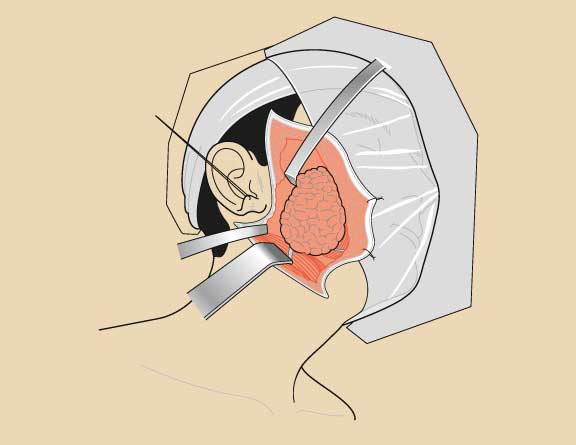
- Hidden incisions: Small cuts behind the ear and in the hairline or through a retroauricular approach. Scar sits where hair grows over it or behind the ear where nobody sees it. Patient walks out of hospital without a visible mark on the side of their face.
- Remote access dissection: Surgeon creates a working tunnel from the incision site to the parotid gland under the skin flap. Da Vinci robotic arms enter this space with 3D magnified view and wristed instruments reaching the gland from behind instead of through the front.
- Facial nerve identification: The nerve runs through the parotid gland splitting into five branches controlling forehead movement, eye closure, smile, and lower lip function. Robotic magnification makes identifying each branch easier than the naked eye view open surgery provides in a bloody field.
- Gland removal: Superficial or total parotidectomy depending on tumor location and pathology. Specimen comes out through the hidden incision intact for proper pathological assessment. Oncological clearance matches open surgery with the cosmetic advantage of no visible facial scar.
Your oncologist assesses robotic parotidectomy suitability based on tumor size and location through parotid cancer evaluation protocols.
Who Needs Parotidectomy ?
Not every parotid lump needs surgery. But when it does the decision between open and robotic approach depends on tumor type, size, and where exactly it sits within the gland.
- Parotid tumors: Pleomorphic adenoma is the most common benign parotid tumor and it needs removal because leaving it carries a small but real long-term malignant transformation risk. Warthin’s tumor is the second most common and some of these can be watched if small and asymptomatic.
- Parotid cancers: Mucoepidermoid carcinoma, adenoid cystic carcinoma, acinic cell carcinoma. These need total parotidectomy with facial nerve preservation when the nerve isn’t invaded. Robotic approach achieves this with better cosmesis but the decision to use it depends on whether tumor extent allows remote access safely.
- Growing or symptomatic lumps: Parotid mass that’s growing on serial ultrasound or causing facial pain needs FNAC at minimum. If cytology shows neoplasm, surgery follows because waiting for a parotid tumor to declare itself as malignant through rapid growth or facial nerve palsy means you waited too long.
- Facial nerve considerations: Tumor stuck to the facial nerve or causing pre-operative facial weakness usually needs open access because the surgeon may need to sacrifice and graft the nerve. Robotic remote access works best when the nerve is uninvolved and the goal is preservation not reconstruction.
Understanding how IORT breast treatment delivers targeted therapy through precision technology helps appreciate why robotic parotidectomy follows the same principle of better outcomes through smarter surgical access.
Why Choose MACS Clinic?
Dr. Sandeep Nayak performs robotic parotidectomy as part of a comprehensive head and neck cancer surgery program that also includes TORS, RABIT, MIND, and RIA-MIND all under one team. MACS Clinic handles FNAC, imaging, surgical planning, and the operation itself without patients being shuffled between departments that don’t talk to each other.
Parotid tumor patient walks in here and gets an honest assessment of whether robotic approach works for their specific case. If the tumor allows it, they get scarless surgery. If it doesn’t, they get told why instead of discovering mid-operation that the plan changed.
FAQs
Does robotic parotidectomy leave a visible scar?
No, incisions hide behind the ear or hairline with no scar on the face.
Is the facial nerve safe during robotic parotidectomy?
Yes, robotic magnification improves nerve identification and preservation rates.
What is the most common parotid gland tumor?
Pleomorphic adenoma, a benign tumor that still requires surgical removal.
How long does robotic parotidectomy take?
Typically 2-3 hours depending on tumor size and whether total parotidectomy is needed.
References
- Salivary gland tumors and treatment — National Cancer Institute
- Parotid surgery guidelines — World Health Organization